Gaps in Health Policy Framework
Although Kerala published a State Health Policy in 2019 (in Malayalam), the document is not available in the public domain and has not been operationalised through an updated, comprehensive policy framework. This absence is increasingly concerning given the scale and complexity of health challenges facing the state.
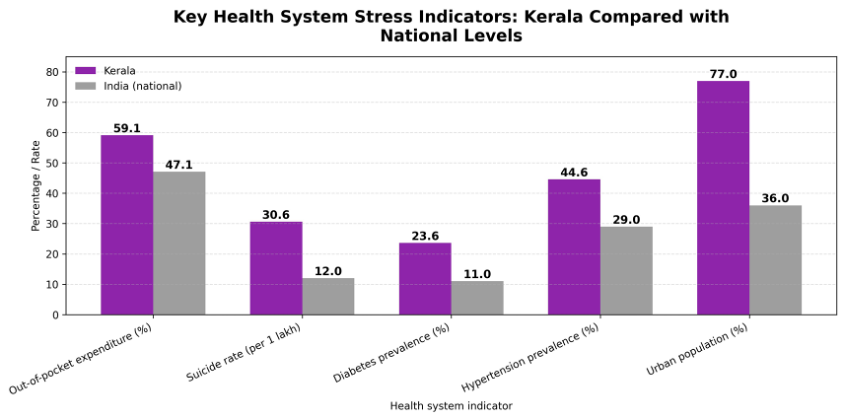
Kerala is experiencing rapid population ageing, with nearly 16% of residents aged over 60 years, alongside a high and growing burden of non-communicable diseases and injuries. Diabetes prevalence is estimated at around 20%, mental health conditions affect over 11% of the population—exceeding national averages—and road traffic injuries claim more than 4,000 lives annually.
At the same time, the state faces emerging and re-emerging infectious disease threats, as highlighted during the COVID-19 pandemic, increasing privatisation of healthcare (particularly in maternity care), climate-related health risks, and rising human–animal conflict.
Despite these converging pressures, Kerala currently lacks an updated and publicly articulated Health Policy that responds to present-day realities and is explicitly aligned with Sustainable Development Goal 3 and Universal Health Coverage (UHC) commitments. The absence of such a policy has resulted in a fragmented strategic landscape, with no clear, overarching vision to guide system-wide reforms, prioritisation, and long-term investment in health and well-being.
In the absence of a comprehensive health policy, the state’s response has largely relied on programme-based initiatives such as the Aardram Mission. While such initiatives have contributed to service delivery improvements, they function as implementation programmes rather than as substitutes for a coherent policy framework.
Programme-led approaches, when not anchored within an overarching health policy, risk reinforcing fragmentation and limiting progress towards UHC by focusing on discrete interventions rather than system-wide transformation.
Kerala enacted the Kerala Public Health Act in 2023, which provides a legal framework for public health regulation and enforcement. However, the Act does not constitute a health policy and does not articulate a comprehensive vision for health system development, financing, equity, or accountability, nor does it explicitly recognise health as a human right.
To date, the state has not issued a formal justification for the absence of an updated, comprehensive Health Policy, despite repeatedly referencing programmes such as the Aardram Mission, expansions under government-funded insurance schemes (KASP, MEDISEP), and the Public Health Act as proxies for policy direction.
A comprehensive Health Policy is essential to define strategic priorities, clarify governance and accountability arrangements, integrate public and private sectors, address emerging health risks, and guide sustainable financing and workforce planning.
The continued absence of such a policy undermines coherence, transparency, and public confidence, and limits the state’s ability to respond systematically to Kerala’s evolving health challenges.
2.1 Disease Burden and Emerging Health Risks
Communicable Diseases
- Diarrhoeal diseases: Kerala reported 5.25 lakh cases of acute diarrhoeal disease in 2025, with 10 deaths (As per state surveillance data – IDSP, 2025). This sustained burden reflects persistent gaps in water quality and sanitation. Seasonal outbreaks continue to strain Primary Health Centres (PHCs), highlighting persistent gaps in sanitation infrastructure and disease surveillance.
- Hepatitis A: In 2025, the state recorded 19,297 suspected cases and 12,378 confirmed cases, with 69 deaths. Outbreaks remained concentrated in districts such as Malappuram and Ernakulam, with adult populations disproportionately affected. Despite vaccine availability, Hepatitis A is not part of the routine immunisation programme, underscoring gaps in targeted vaccination, drinking water safety, and sewage management.
- Chickenpox: Kerala reported 29,055 confirmed chickenpox cases in 2025, with 10 deaths. Suspected cases are not reported separately. The absence of the vaccine from the national immunisation schedule has contributed to recurrent outbreaks, particularly among school-age children, placing avoidable pressure on primary care services.
- Tuberculosis (TB): Over 21,500 new TB cases were identified in 2023, with approximately six deaths reported daily. While Kerala has made notable progress in TB control, drug-resistant TB and high comorbidity with diabetes continue to pose challenges, placing sustained pressure on diagnostic, treatment, and follow-up capacity.
Non-Communicable Diseases (NCDs)
- Cardiovascular diseases: Heart attacks and strokes are the leading causes of death in Kerala, accounting for 26 percent of all deaths. Ischemic heart disease is the top contributor to early mortality, followed by stroke. Alarmingly, 60 percent of male and 40 percent of female cardiac deaths occur before the age of 65. Recent studies also show that 25 percent of heart attack victims in Kerala are under the age of 30, indicating a growing crisis of premature cardiovascular disease.

- Diabetes mellitus: An estimated 23.6% of adults in Kerala live with diabetes, while 18.1% have pre-diabetes, nearly double the national average, positioning the state among the highest-burden settings for diabetes in India (ICMR-INDIAB study). The rising prevalence has increased complications such as kidney failure, heart disease, and amputations, increasing the cost and complexity of care. The system faces growing demand for insulin, dialysis, and patient follow-up, while preventive strategies such as nutrition and physical activity remain under-addressed.
- Hypertension: Approximately 44.6% of adults in Kerala have hypertension, with a substantial proportion remaining undiagnosed or inadequately controlled (ICMR-INDIAAB study). These gaps in detection, treatment adherence, and follow-up contribute to preventable cardiovascular events, including heart attacks and strokes.
- Cancer: Kerala has recorded a 54 percent increase in cancer cases over the past decade, from 39,672 in 2015 to 61,175 in 2024. Thiruvananthapuram reports one of the country’s highest breast cancer rates. Common cancers include breast, oral, lung, and colorectal types. As incidence rises, the public health system is under growing pressure to expand screening, enhance treatment capacity, and reduce the financial burden on families.

- Obesity and lifestyle risks: Sedentary behaviour, unhealthy diets, and physical inactivity are driving obesity and related metabolic disorders. Kerala has emerged as the state with the highest prevalence of abdominal obesity, affecting an alarming 65.4 percent of women. Though often under-recognised, obesity is a growing public health issue in the state, among adults, adolescents, and children. It is closely linked to rising rates of diabetes, hypertension, and heart disease. Preventive and lifestyle-modification efforts remain uneven and under-scaled.
Vector-borne and Zoonotic Threats
- Dengue fever: In 2025, Kerala reported 29,300 suspected dengue cases and 10,886 confirmed cases, with 56 reported deaths. Seasonal surges are straining vector control systems and hospital capacity as urbanisation and climate change create favourable breeding conditions for mosquitoes.
- Leptospirosis: During 2025, Kerala recorded 2,258 suspected cases and 3,469 confirmed cases, with 223 reported deaths. Flooding, poor drainage during the monsoon, and unsafe occupational exposures fuel recurrent outbreaks. Delayed diagnosis and critical care constraints contribute to high fatality rates, particularly in flood-prone districts.
- Nipah virus: Since 2018, Kerala has experienced multiple Nipah virus outbreaks. In 2025, the state reported 4 confirmed Nipah cases, including 2 deaths. The virus’s high fatality rate and outbreak potential underscore the need for sustained preventive measures, rapid emergency response mechanisms, adequate ICU capacity, and close coordination across human, animal, and environmental health sectors. Nipah virus is recognised by the WHO as a pathogen with epidemic and pandemic potential.
- Scrub typhus: In 2025, Kerala reported 158 suspected cases and 864 confirmed cases, resulting in 13 deaths. This mite-borne infection is expanding beyond rural pockets into urban and hilly regions. Delayed detection highlights gaps in diagnostics and fever case management, reinforcing the need for stronger primary care and surveillance systems.
Nutritional Health
- Anaemia: Anaemia remains a persistent public health issue in Kerala, especially among women and children. As per National Family Health Survey-5 (NFHS-5), over 30% of women of reproductive age are anaemic. This reflects ongoing gaps in iron supplementation, food diversity, and nutrition education.
- Vitamin deficiencies: Micronutrient deficiencies are widespread across age groups. As per the Comprehensive National Nutrition Survey (CNNS), nearly 27% of school-aged children show signs of vitamin A deficiency, and around 32% of adolescents and 12% of pre-schoolers have vitamin D deficiency. Vitamin B₁₂ deficiency affects nearly half of adolescents.
- Malnutrition: Kerala faces a dual burden of undernutrition and obesity. Around 23% of children are stunted, 16% are wasted, and 20% are underweight. At the same time, 4% of under-5 children and 38% of adult women are overweight or obese.
- Poverty and food insecurity as underlying determinants: Kerala still has around 5.9 lakh Antyodaya Anna Yojana households, indicating continued dependence on subsidised food systems.
- Dietary quality, affordability, and nutrition inequities: Limited dietary diversity and rising food prices disproportionately affect women, children, older adults, and tribal populations.
Mental Health
- Mental illness: An estimated 11.3% of the population experiences mental health conditions.
- Suicide: Kerala has one of the highest suicide rates in India—about 30.6 per 1 lakh population—with over 10,970 deaths reported in 2023.
- Substance use: Around 12.4% of the population consumes alcohol. In 2024, Kerala recorded 27,701 cases under the NDPS Act.
- Adolescent mental health: Over 60% of adolescents show symptoms of depression or anxiety. School-based mental health support remains severely inadequate.
Emerging Systemic Threats
- Antimicrobial Resistance (AMR): AMR is a growing public health threat. While Kerala has led containment efforts through KARSAP and Operation AMRITH, gaps remain in prescription oversight and OTC dispensing control.
Injuries and Trauma
- Road traffic injuries: In 2024, Kerala reported 48,919 road traffic accidents and 3,774 deaths. In 2025 (up to November), the state recorded 45,543 accidents and 3,365 deaths, underscoring ongoing pressure on trauma systems.
2.2 Infrastructure, System Resilience, and Governance
Gaps in Public Health Facilities
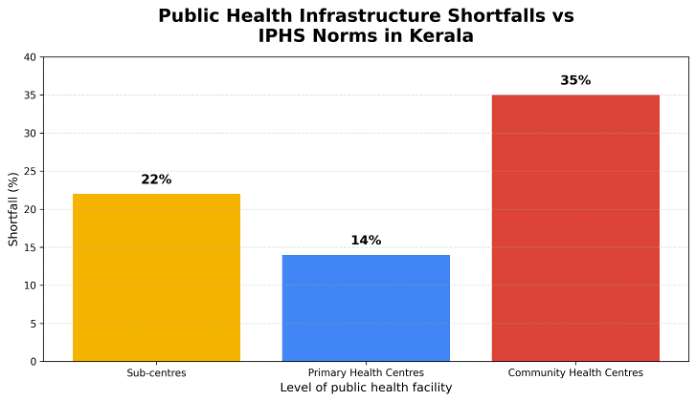
- Shortfall in primary care facilities: As highlighted in the CAG Performance Audit (2024), Kerala continues to face a substantial shortfall in frontline public health infrastructure. There is a 22% shortfall in Sub-Centres (SCs) and a 14% shortfall in Primary Health Centres (PHC) compared to prescribed norms. The deficit is more pronounced at the secondary level, with a 35% shortfall in Community Health Centres (CHC). Districts such as Malappuram and Idukki remain particularly under-served. Only two districts meet PHC norms and just one meets SC norms, revealing persistent geographic inequities in access to basic public healthcare. These infrastructure gaps leave rural, coastal, and remote populations with limited access to timely primary care, increasing avoidable referrals and dependence on higher-level facilities.
- Urban primary care: Despite Kerala’s strong aggregate health indicators, urban areas remain significantly underserved by the public primary care system. As of early 2025, the state has 102 Urban Primary Health Centres (UPHCs) and only 2 Urban Community Health Centres (UCHCs), covering just 58 of 93 urban local bodies. Over one-third of municipalities lack even a single UPHC. Only 29% of urban wards and 18% of the urban population are covered under the National Urban Health Mission (NUHM). This gap disproportionately affects urban poor, informal-sector households, and migrant workers, who are often compelled to rely on private clinics and hospitals for routine care, thereby increasing out-of-pocket expenditure even for minor ailments.
- Access gaps in tribal and remote areas: In tribal and hilly regions such as Attappady, public health infrastructure remains limited despite Kerala’s longstanding commitment to universal health coverage. The Attappady valley, home to approximately 30,000 tribal residents, is served by only two PHCs, one CHC, and a single Tribal Specialty Hospital. Most tribal hamlets lack even a sub-centre. In one widely reported instance, a pregnant woman was forced to be carried nearly 16 kilometres on foot, resulting in a stillbirth due to delayed access to care. These areas continue to face weak road connectivity, limited ambulance availability, and thinly staffed facilities, reflecting persistent structural neglect in health-system planning for geographically and socially vulnerable populations. People who suffer from emergencies due conditions such as accidents, heart attack, stroke or complicated delivery most often rush to private healthcare facilities in Coimbatore city in Tamil Nadu State disregarding the district-level tertiary care facilities at Palakkad town due to the bad condition of the roads to Palakkad. This causes out-of-pocket spending for the transportation and treatment. For visiting Attappady recently, it’s reported that, the health minister also avoided the Kerala roads and took the route via Coimbatore.
- Shortfall in secondary care facilities: The latest CAG Performance Audit shows serious shortfalls in secondary-care facilities. The Executive Summary records a 35% shortfall of CHCs compared with IPHS norms in the State. Of 5,332 health-infrastructure works approved during 2016–22, only 1,304 (24.45%) were completed; for secondary hospitals specifically, just 1 of 46 (CHC)/District Hospital (DH)/ Sub- District Hospital (SDH) – also called Taluk Hospital (THQH) works (2%) and 16 of 50 CHC works (32%) were completed, with the rest dropped or not started. In terms of beds, 16 of 19 District Hospitals had beds below IPHS norms and in 11 of these 16 DHs the deficiency was more than 40%. Many test-checked SDHs and CHCs lacked adequate or safe buildings, with some SDH buildings declared unsafe but still in use and several CHCs functioning from old or inadequate buildings, further weakening secondary-care service delivery.
- Shortfall in tertiary care facilities: The latest CAG Performance Audit report shows major shortfalls in tertiary care capacity. Of the new government medical college projects planned as tertiary centres, only one was fully completed by the cut-off date, while others remained around 70–90% complete, limiting the intended expansion of tertiary beds and services. In at least one medical college, only about 60–65% of sanctioned inpatient beds were operational due to incomplete buildings and support infrastructure. Critical tertiary units such as burns units, trauma/ICU facilities and key equipment (including sufficient functional ventilators) were either delayed, not fully equipped or non-functional, leading to under-utilisation of nominal ICU and specialty capacity. Trivandrum medical college, the first medical college in Kerala, face shortages in staff, beds, equipment, ICU facilities and even ventilators.
- Limited maternity and specialty services at local facilities: A large proportion of PHCs and CHCs lack the infrastructure, equipment, and trained personnel required to provide basic maternity care or essential specialist services. Consequently, more than 60% of deliveries in Kerala now take place in private hospitals, even when antenatal care has been provided through government facilities. This pattern reflects not only service limitations at public institutions but also declining public confidence in the availability of emergency obstetric care at local government facilities. The resulting shift towards private institutions significantly increases household expenditure on childbirth and postnatal care.
Hospital Capacity Constraints and Uneven Bed Distribution
- Unsafe and ageing public health infrastructure: A significant share of Kerala’s public health infrastructure is operating under unsafe conditions. Audit findings and official assessments have identified over 225 buildings across 134 government hospitals as structurally unsafe or at risk of failure.
- Overcrowding and bed shortages in tertiary hospitals: Kerala’s major public hospitals operate far beyond sanctioned capacity. For instance, the Medical College Hospital (MCH) in Thiruvananthapuram functions at over 170% occupancy.
- Long waits for treatment and critical care: Backlogs for surgeries and specialised procedures are common. At Thrissur medical college, more than 400 cardiac patients remain on waiting lists due to the presence of only a single active cardiac surgeon.
- Bed capacity meets national norms but lags behind needs: Though Kerala has a hospital bed ratio of approximately 1.2 beds per 1,000 population, it remains inadequate considering the morbidity pattern and health-seeking behaviour.
- Systemic referral issues exacerbating overcrowding: Weak coordination between primary, secondary, and tertiary facilities significantly contributes to congestion at medical colleges.
Fragile Emergency Care and Referral Transport Systems
- Gaps in trauma and emergency care infrastructure: Most government hospitals lack dedicated trauma care units or emergency surgery facilities.
- Referral transport and inter-facility coordination gaps: Families frequently bear the responsibility of moving patients between facilities due to inconsistent ambulance support.
- Limited emergency response capacity in the public sector: The ‘108 Kerala Emergency Medical Services Project (KEMP)’ faces persistent coverage gaps, particularly in rural, coastal, and hilly areas.
- Operational and funding challenges affecting ambulance services: By late 2024, unpaid dues led to state-wide strikes by ambulance personnel, disrupting services.
- Referral transport and inter-facility coordination gaps: Inefficient referral chains contribute to tertiary-level overcrowding and reliance on private emergency services.
Governance, Decentralisation, and Coordination Gaps
- Overlapping responsibilities and dual control: Kerala’s decentralised health system continues to suffer from blurred accountability between local governments and state-controlled staff.
- Underutilisation of Panchayati Raj Institutions (PRIs) and health funds: More than half of health-sector grants available to local bodies remained unutilised or delayed in use.
- Weak intersectoral coordination affecting disease prevention: Recent communicable disease outbreaks have highlighted gaps in coordinated action across departments.
- Budgetary and institutional rigidity limiting local action: Health accounted for about 5.5% of total state expenditure in 2024–25, limiting fiscal space for reform.
- Weak accountability, oversight, and implementation capacity: System audits have pointed to persistent governance failures in procurement and infrastructure management.
Limited integration of disaster preparedness within health governance: Kerala faces rising climate-related risks including floods, landslides, heat stress, and monsoon-linked disease outbreaks. District- and local-level health institutions vary widely in readiness, reflecting gaps in embedding disaster risk management within regular health governance processes.